Choosing Between Modifier 53 And 52 (Gastroenterology Example)

By definition, modifier 53 is used to indicate a discontinued procedure and modifier 52 indicates reduced services. In both the cases, a modifier should be appended to the CPT code that represents the basic service performed during a procedure.
Choosing between modifiers 53 and 52 can sometimes be confusing. A wrong modifier can lead to denials. The reason for this confusion is the ambiguity in its definitions.
American Medical Association (AMA) clarified these definitions in the CPT manual (Refer to CPT 2018 Professional Edition) page # 314 where it outlines clear guidelines on usage of modifier 53 and 52.
In gastroenterology, separate rules are created for upper and lower GI procedures.
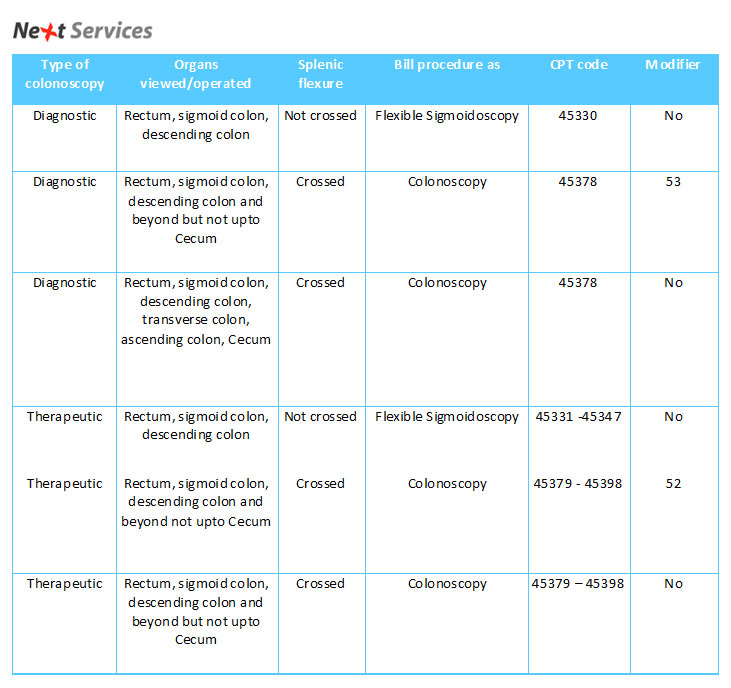
For example, whenever a colonoscopy is performed, it is necessary to determine if the colonoscopy is performed for diagnostic purpose or a therapeutic reason. While coding, medical documentation should be referred to for specific modifier usage cues.
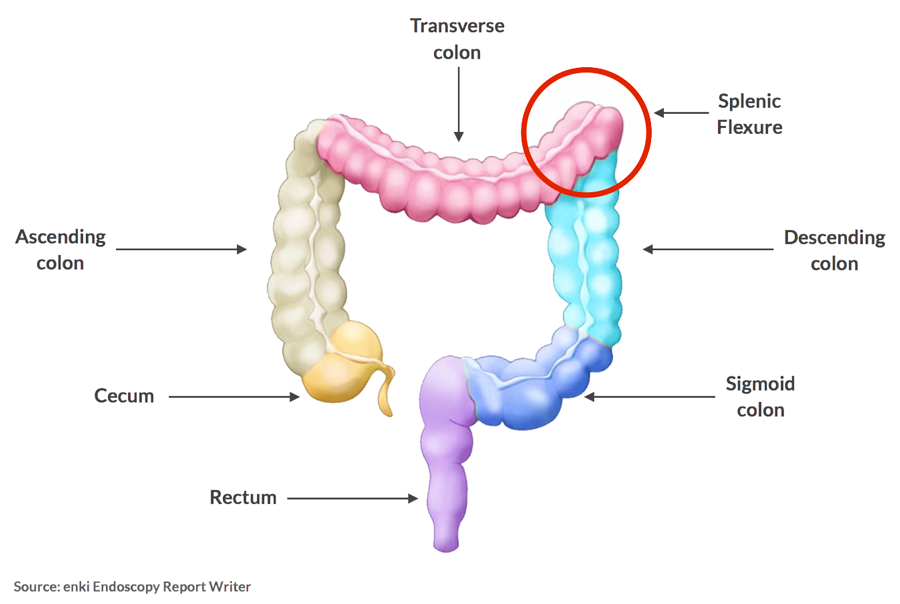
Medical documentation should indicate the part of the colon till the scope could be advanced. Please refer to the diagram below for anatomical positions of important parts of colon.
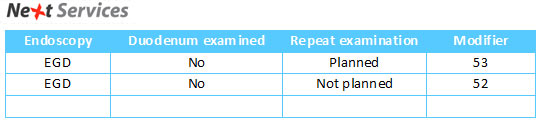
CPT 2018 Professional Edition also defines the usage of modifiers 52 and 53 in EGD. The use of modifier 52 or 53 is based on scheduling a repeat EGD. Refer to the chart for using modifiers during EGD.
Using wrong modifiers leads to underpayments and in many cases, claim denials. You can avoid problems with your claims by referring to these coding guidelines and paying closer attention to specific case scenarios.
Have you come across a unique coding scenario? How did you get it resolved? Let us know in the comments below.
Disclaimer – CPT® 2018 Professional Edition is the definitive AMA authored resource to help health care professionals correctly report and bill medical procedures and services. The AMA publishes the only CPT® codebook with the official CPT guidelines.
The information is presented for educational use only. It is not meant to be used to diagnose or treat any medical condition. We have made all reasonable efforts to ensure the information provided in this guide is accurate at the time of inclusion, however, please resort to clinical documentation and your experience to make decisions while coding and billing for procedures.
1. [FREE GUIDE] CPT CODES FOR ENDOSCOPY PROCEDURES
Remembering codes with so many permutations and combinations can be really overwhelming. To help you understand and code better, we have created this reference guide which you can refer to code and bill accurately for your next case. Guide includes CPT Codes for Colonoscopy, Esophagoscopy, EGD, Enteroscopy, ERC and Sigmoidoscopy.
2. [FREE GUIDE] ICD-10 CODING GUIDELINES FOR SCREENING & SURVEILLANCE COLONOSCOPY
October 1st, 2016 marked the end of the grace period allotted by CMS and AMA to facilitate smooth ICD-10 implementation. During the grace period, insurances processed claims even if they were wrongly coded, just as long as the codes belonged to the broader family of correct codes. However, such claims will not be paid after the grace period. It now becomes crucial for medical practices to strictly adhere to ICD-10 coding guidelines to avoid payment disruptions.
Guide includes ICD-10 Coding guidelines for screening and surveillance colonoscopy.